 Fire & EMS Leader Pro The job of old firefighters is to teach young firefighters how to become old firefighters!
Fire & EMS Leader Pro The job of old firefighters is to teach young firefighters how to become old firefighters!
By: Dr. Kristen Wheldon, Psy.D and Battalion Chief (Ret.) Robert Avsec
A time-worn adage in the fire service is “200 years of tradition, unhampered by progress.” In some situations that might be true and in this article, you’ll see just how time-worn, and incorrect, those words truly are.
Changes to EMS Care
The first fire-based paramedic programs in the U.S. were implemented in the late 1960s and early 1970s. Since those first programs were launched, quite a few of the treatment modalities for paramedics have evolved over time, reflecting advancements in medical knowledge, technology, and best practices. Let’s look at just a few of those things that have changed in EMS over the last 60+ years, starting with treatment modalities introduced over the years.
- Point-of-Care Ultrasound. Paramedics now often use portable ultrasound devices to quickly assess conditions like internal bleeding or cardiac tamponade on the spot.
- Rapid Sequence Intubation. This procedure, involving sedation and paralysis to place an endotracheal tube, to protect an unconscious patient’s airway, has become more common.
- Pre-hospital Blood Transfusion. In a growing number of fire and EMS departments, paramedics can give blood transfusions to hypovolemic shock patients before reaching the hospital.
When we look at treatment modalities eliminated or reduced for EMS providers, we can see many changes that have been made to improve patient outcomes.
- Routine Use of Spinal Immobilization. Research has shown that rigid immobilization may do more harm than good, leading to a reduction in its usage.
- Use of Backboards. Similarly, the use of backboards is now limited as they can cause pressure sores and respiratory impairment.
- Hyperventilation in Cardiac Arrest. Previously used, now reduced due to its adverse impact on blood flow to the heart and brain.
- Military anti-shock trousers (MAST). Initially used for the treatment of patients experiencing hypovolemic shock, MAST is no longer used as the research showed no significant benefit.
- Sodium bicarbonate. The routine administration of sodium bicarbonate during cardiac arrest resuscitation efforts was the standard of care until research indicated that giving it without first measuring a patient’s acid/base balance was potentially harmful.
- CPR. And how many times over the years have the protocols for CPR changed?
These changes were aimed at improving patient outcomes and reflected a growing body of research-based evidence for pre-hospital care.
Read Next: Who sets standards for pre-hospital emergency care?
Changes in How We Suppress Fires
EMS is not the only service provided by fire departments that has seen changes based on research. Fire behavior research by UL (Underwriters Laboratories) and NIST (National Institute of Standards and Technology) has significantly influenced modern firefighting techniques in the U.S. Here are some key impacts from their research.
- Improved Understanding of Fire Dynamics. Research by UL and NIST has provided valuable insights into how fires spread within structures (i.e., the flow path). Firefighters are now better trained to recognize and control flow paths, reducing the risk of backdrafts and flashovers.
- Ventilation Strategies. Positive Pressure Ventilation (PPV) studies have shown that PPV can effectively control and exhaust fire gases, improving visibility, and reducing heat. Firefighters are now trained to use PPV strategically to enhance occupant and firefighter safety.
- Modernizing Tactics for Fire Suppression. Research has highlighted the effectiveness of using a transitional attack (initially attacking the fire from the outside before moving inside) to quickly knock down flames and “reset” the interior heat conditions to increase the potential for survivability for building occupants and reduce heat stress to firefighters entering the structure. Many fire departments have adopted this as a standard fire suppression tactic.
- Better Fire Suppression Techniques. Water Mapping studies have demonstrated the pros and cons of various water application methods, contributing to more effective fire suppression. This includes understanding the patterns and impacts of different hose streams.
- Building Construction Materials. UL’s research on modern building construction materials (e.g., lightweight trusses and engineered lumber) has shown their potential for rapid failure under fire conditions, leading to changes in firefighting strategies when dealing with such structures.
- Practical Influence on Firefighting. Fire academies and fire departments have incorporated the findings of UL and NIST into their training programs to ensure that firefighters are better prepared for modern fire environments. Fire safety standards (e.g., NFPA standards) and fire department policies have been updated based on this research to improve overall fireground safety and efficiency.
Ultimately, the ongoing research by UL and NIST ensures firefighters have the latest knowledge and tools to combat fires effectively while prioritizing safety for themselves and the communities they serve.
Firefighter Mental and Behavioral Health
So, we know that fire service organizations and fire departments can make changes based upon research-based evidence that’s been developed by non-fire service organizations. Why then are fire departments and the major fire service organizations loathe to seek guidance and direction for the critical mental and behavioral health issues faced by firefighters (e.g., post-incident stress, suicide) from the psychology profession, the non-fire service organization with the requisite knowledge, skills, and experience needed to develop proactive strategies to address those issues?
From here, I’ll turn the helm over to Dr. Kristen Wheldon, Psy.D, a licensed psychologist in California and the founder of the Fire Service Psychology Association in 2017.
The “Train”
Efforts to understand the psychological effects of war and trauma date back centuries, with accounts even found in Homer’s Odyssey, where Odysseus is depicted experiencing anger, memory loss, compulsive tendencies, and violent behavior—symptoms that often align with what we now recognize as post-traumatic stress. From the battlefields of ancient Greece to modern war zones and fire grounds, society has been on an evolving journey, attempting to grasp the true nature of psychological wounds.
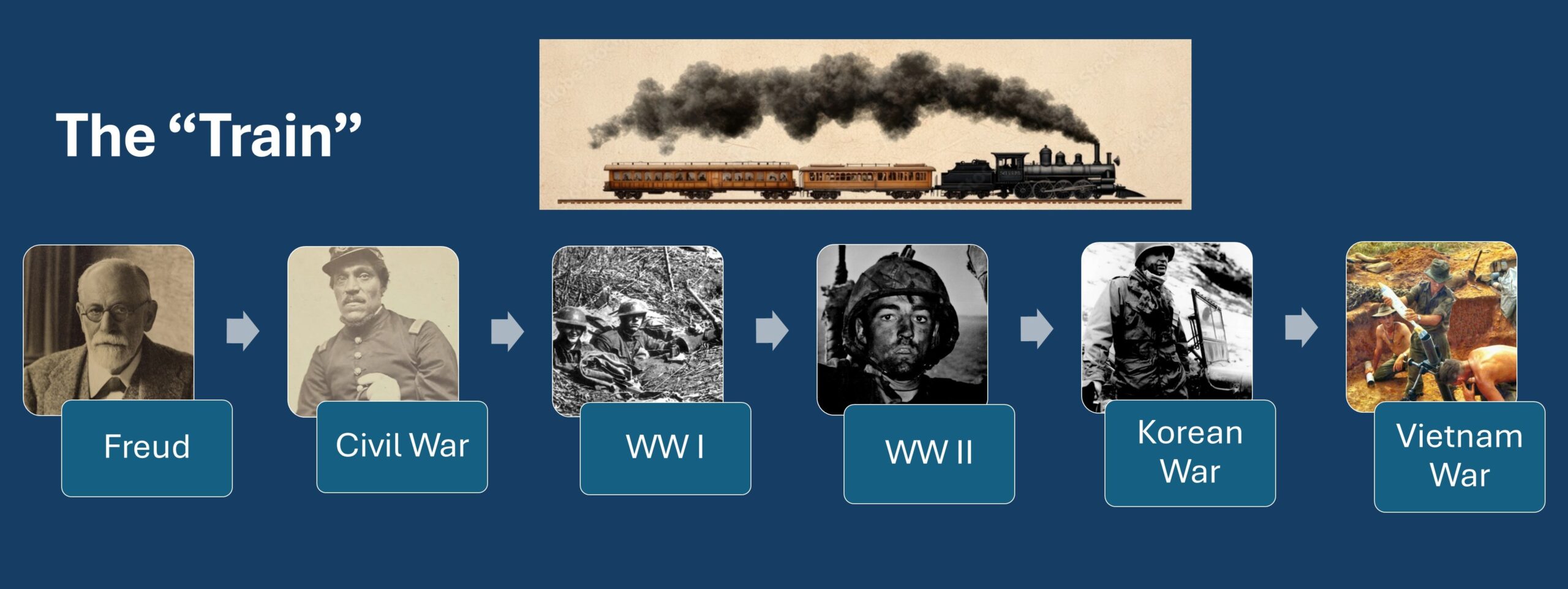
That process is akin to a train moving through time, making stops at key moments in history as our understanding of PTSD evolves. Once seen through the lens of Freudian repression—where trauma was thought to stem from unresolved childhood conflicts, the prevailing view has shifted. PTSD is now understood as a fear-based conditioning model, where exposure to life-threatening events has the potential to rewire the brain, leaving individuals trapped in cycles of hyperarousal, avoidance, and distress.
The train left its first major station in the 1860s, during the Civil War and Franco-Prussian War. Soldiers stricken with Nostalgia or Soldier’s Heart were viewed as weak, cowardly, or simply homesick. Many were executed, others deserted, and some found ways to serve in non-combat roles, such as medics and engineers. The idea that exposure to trauma could fundamentally alter a person’s psychological state was only just beginning to take shape.

During World War I, the train stopped at Shell Shock, where Dr. Thomas Salmon pioneered one of the first structured responses to combat stress. He found that treating soldiers near the sound of the guns and giving them food, rest, and reassurance resulted in a 75% return-to-duty rate. This approach demonstrated that early intervention could mitigate long-term psychological harm.
The term Battle Fatigue emerged as the train pressed on through World War II. Mental health professionals, though few in number, attempted to refine treatment, but their efforts were often constrained by bureaucracy and outdated theories. Soldiers suffering from psychological wounds were sometimes misdiagnosed, over-medicated, or dismissed as malingerers. Screening processes became a double-edged sword—some were wrongly deemed unfit for service, while others were overlooked entirely.

By the Korean War, Dr. Albert Glass applied hard-earned lessons from previous conflicts, refining the PIES principles:
- Proximity – Treat close to the front
- Immediacy – Intervene as soon as symptoms appear
- Expectancy – Instill confidence in recovery
- Simplicity – Focus on rest, nutrition, and support
This approach proved highly effective, with over 90% of soldiers returning to duty after receiving psychological first aid.

However, the train took a sharp detour during the Vietnam War, where the military misapplied past lessons. Combat fatigue was either ignored or misunderstood, leading to over-medication, misdiagnosis, and even cases where soldiers suffering from major mental illnesses like psychosis or bipolar disorder were returned to duty. The failure to adequately support veterans led to a significant increase in post-war psychological distress.
By the 1980s, as the train neared another critical junction, the world began moving toward Psychological First Aid (PFA). This flexible, evidence-based approach emphasized resilience, social support, and voluntary intervention. Research increasingly questioned the effectiveness of Critical Incident Stress Debriefing (CISD), a structured group intervention that required individuals to relive traumatic events shortly after they occurred. Studies showed that this approach could sometimes do more harm than good, increasing distress rather than alleviating it.
At this critical moment, the fire service took a different track. While military forces, mental health organizations, and researchers embraced PFA, fire departments fully adopted Critical Incident Stress Management (CISM), embedding CISD into their standard protocols. Unlike the rest of the world, which adapted based on new research, the fire service remained committed to a method that studies increasingly challenged.
As the train moved into the 1990s and 2000s, research continued to highlight the limitations of CISD. The U.S. military, the VA, the National Center for PTSD, and global health organizations all reinforced the need for voluntary, individualized interventions rather than mandatory debriefings. By 2017, the American Psychological Association formally recommended against CISD, emphasizing the effectiveness of Psychological First Aid instead.
Yet, despite these shifts, the fire service remained on its separate track. The methods that were once considered best practice in the 1980s had since been revised, but many fire departments had not updated their approach.
As the train continues, the fire service stands at a crossroads. Will it merge onto the track, aligning with current research and embracing PFA with evidence-based screening methods such as Trauma Risk Management? Or will it remain at the outdated station, relying on methods left behind by military and mental health professionals alike?
One thing is sure—the train isn’t stopping. New generations of warriors, first responders, and firefighters will continue to face trauma, and how we respond will determine how well they recover. The choice is ours: Should we stay at the old station with our 1980s understanding of trauma response or move forward with the evolving science of evidence-based practice?
About the Co-Author
Dr. Kristen Wheldon, Psy.D, is a licensed clinical psychologist in private practice in Southern California. She’s the founder and president of the Fire Service Psychology Assocation, and organization of fire service leaders, psychologists, and masters-level clinicians working to “bridge the gap between professional psychology and the fire service.”