 Fire & EMS Leader Pro The job of old firefighters is to teach young firefighters how to become old firefighters!
Fire & EMS Leader Pro The job of old firefighters is to teach young firefighters how to become old firefighters!
By: Robert Avsec, Executive Fire Officer
CO poisoning is a significant health risk for firefighters who are exposed to smoke during fire suppression operations. Fire departments must increase their efforts to identify the early on-set of CO poisoning through aggressive assessment of all firefighters post exposure. And that needs to happen in firefighter rehab.
In 2015, the National Fire Protection Association (NFPA) released its updated NFPA 1584: Standard on the  Rehabilitation Process for Members During Emergency Operations and Training Exercises. That revision (the current standard) expanded the medical monitoring requirements for firefighters when they enter an on-scene rehabilitation area.
Rehabilitation Process for Members During Emergency Operations and Training Exercises. That revision (the current standard) expanded the medical monitoring requirements for firefighters when they enter an on-scene rehabilitation area.
Rehabilitation: An intervention designed to mitigate against the physical, physiological, and emotional stresses of fire fighting in order to sustain a member’s energy, improve performance, and decrease the likelihood of [a subsequent] on-scene injury or death (NFPA 1584, 3.3.23).
Know the Requirements for Assessing for CO Poisoning
Most of us are familiar with the basic functions carried out in rehab: cooling (or reheating) of firefighters; rehydration; feeding; and assessment of basic vital signs, e.g., pulse rate, respiratory rate, temperature, and blood pressure readings.
NFPA 1584 now specifies the required vital signs that should be assessed for all firefighters entering rehabilitation. This new requirement includes temperature, heart rate, respiratory rate, blood pressure and pulse oximetry (SpO2) which is a measurement of how well the body’s blood is being oxygenated. In addition, “Members exposed to fire smoke shall be assessed for carbon monoxide poisoning.” (NFPA 1584, 6.2.6.3.2).
The requirement to assess every firefighter for possible CO poisoning can be difficult. The symptoms of CO poisoning are non-specific: headache, nausea, shortness of breath, or gastrointestinal symptoms. In the civilian population, CO poisoning is frequently misdiagnosed initially as food poisoning or a heart attack.
are non-specific: headache, nausea, shortness of breath, or gastrointestinal symptoms. In the civilian population, CO poisoning is frequently misdiagnosed initially as food poisoning or a heart attack.
The use of pulse oximetry is of limited value in assessing a patient’s CO level. NFPA 1584 states that most pulse oximeters are unable to differentiate between oxyhemoglobin [oxygen saturation of hemoglobin in the blood] and carboxyhemoglobin [CO saturation of hemoglobin in the blood] resulting in inaccurate SpO2 measurements (NFPA 1584, (A.6.2.6).
Know the Facts About CO Poisoning
CO and hydrogen cyanide are the two most prominent contaminants present during fire suppression and overhaul activities, hence their label: the “toxic twins.” CO binds aggressively to hemoglobin in the blood reducing its ability to deliver oxygen to critical organs, particularly the heart and brain.
CO poisoning puts firefighters and others at significant risk at the scene of a fire because, as CO in the blood causes 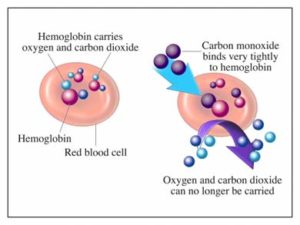 reduced oxygen delivery to the brain, the resultant hypoxia causes mental confusion that can lead to poor decision making. Those individuals who have CO poisoning should receive the appropriate medical care immediately.
reduced oxygen delivery to the brain, the resultant hypoxia causes mental confusion that can lead to poor decision making. Those individuals who have CO poisoning should receive the appropriate medical care immediately.
In the long term, moderate or severe CO poisoning significantly increases an individual’s risk for a myocardial (heart). This is a result of the hypoxia’s impact on the heart muscle. Chronic exposure to CO can cause both long-term cardiac impairment and neurological damage.
CO poisoning can be difficult to detect in the field because no combination of symptoms can be used to confirm or exclude a diagnosis of CO poisoning. Many of us learned in our EMT training that “cherry-red” skin color was a sign of CO poisoning. And while that is true, it is a late sign of CO poisoning and indicates a very high level of CO in the blood with a resultant high level of hypoxia.
The signs, symptoms and diagnosis of acute CO poisoning correlate poorly with carboxyhemoglobin levels in the blood (COHb); without a portable exhaled breath CO monitor, a CO-oximeter (a pulse oximeter designed to measure COHb), or a portable blood gas analyzer an accurate COHb can only be obtained through analysis of a blood sample from the patient and a laboratory analysis (NFPA 1584, A 6.2.6.4(1)
Failure to identify individuals with CO poisoning can have disastrous consequences—so Check Everyone, Every Time!